
Thromboelastography (TEG) is coming to an emergency department near you. For those who rotated at Shock, TEG is utilized to guide administration of blood products during massive transfusion protocol in a bleeding patient. For us, this test will likely be most useful for bleeding in patients on anticoagulation and/or antiplatelet agents.
INR and aPTT only measure the enzymatic clotting time, which means they only measure clotting cascade up until fibrin. Utilizing these tests, it is impossible to know the causes(s) of coagulopathy in intracranial hemorrhage or GI bl er the last time the took their meds.
TEG is a whole blood test and assays clot formation, mechanical strength and stability across time. This allows interpretation of the curve to determine the cause of coagulopathy. Old TEG machines measured the mechanical elasticity and strength of the clot by physically interacting with whole blood. The TEG output across time is measured in maximum amplitude, which is a function of dynes of force generated by the elastic clot. This an example of what a TEG curve looks like (Trepani, et al).

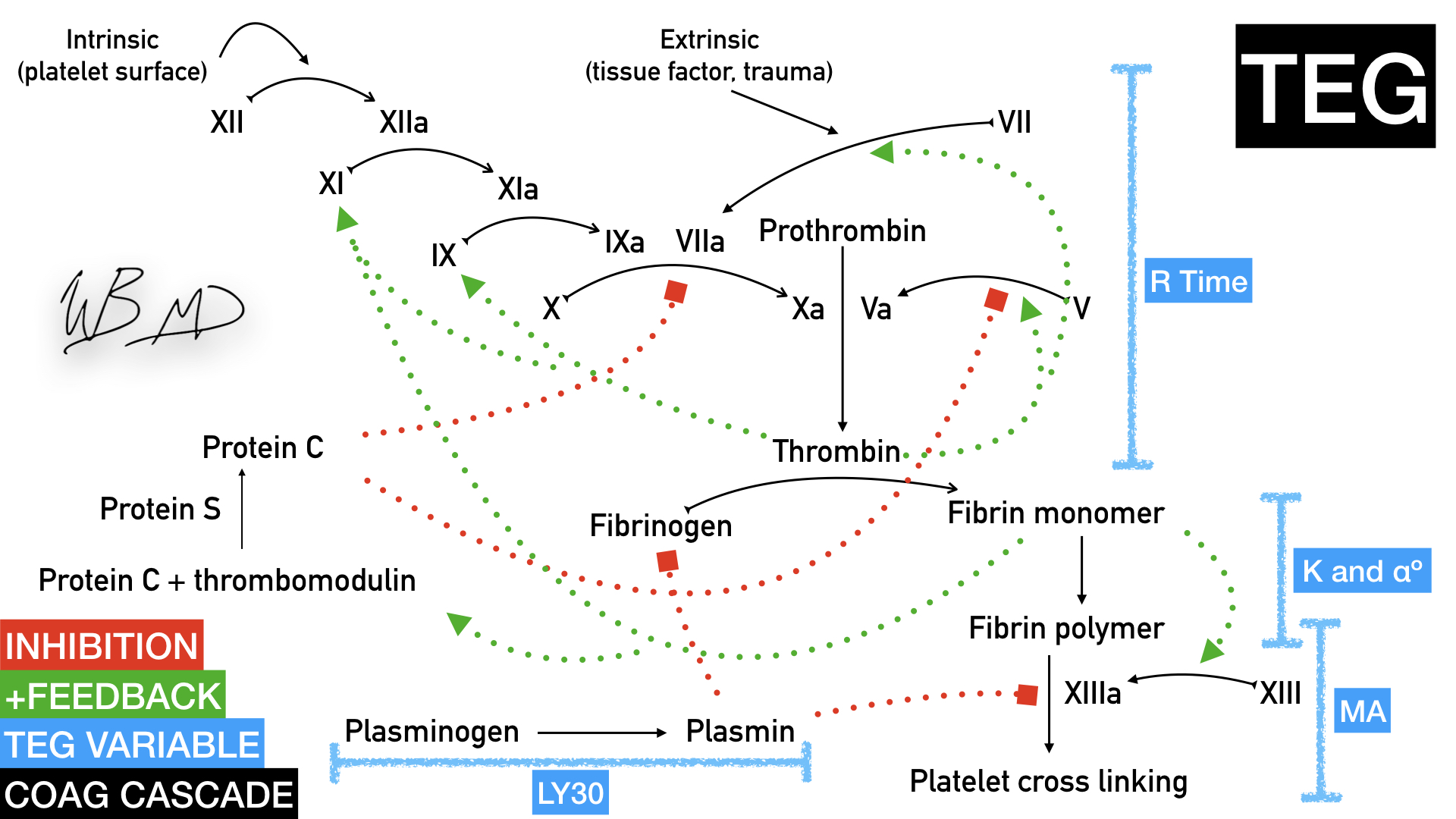
Traditional clotting cascade
Reaction Time R is the time to activation, ending in thrombin. Theoretically any deficiency can cause prolonged R time (eg thrombophilia), but in the setting of trauma, it is most commonly associated with thrombin deficiency. R will also be long with anticoagulation. If R is long, you need praxbind, PCC or FFP depending on the etiology.
Polymerization
Clot Kinetics K is dependent on fibrinogen function and fibrin cross linking
αº is the angle formed between R and the tangent line to the curve at point K.
If either αº or K are low, you can give cryoprecipitate which contains the fibrinogen necessary to correct this coagulopathy.
Clot features
Maximum amplitude (MA in mm) or G (dynes) represents clot strength at its peak. The lower the amplitude, the lower the platelet function. If this is low and patient is bleeding, you need DDAVP or platelets.
LY30 is the amount of clot lysis 30 minutes after MA is achieved, and represents the amount of thrombolysis due to factors in the patient’s blood sample.
Here is a diagram with each of the variables as they relate to the coagulation cascade. Abnormalities in these values suggest the possible cause of their coagulopathy:
TEG 6s
Previous machines analyzed the thromboelastic properties of the clot across time using physical forces. This new generation of machine sends sound waves through 4 channels and measures motion of the sample optically across the clotting time. All 4 tests occur simultaneously in the microfluidic test cartridges. A 5th channel assays platelet function, which we may or may not use.
4 channels:
Kaolin TEG: kaolin is used as an initiation of coagulation cascade. This is channel gives you the classic TEG graph.
Rapid TEG: this channel’s coagulation cascade is rapidly initiated by tissue factor (extrinsic pathway). R will be dramatically shortened because the coagulation cascade is activated faster in this channel.
Heparinase TEG: as the name suggests, this microfluidic channel contains an enzyme that breaks down heparin, which effectively analyzes a heparinized patient’s blood as if they were not on heparin. If the patient is not on heparin the Kaolin TEG and Heparinase TEG should be the same.
Functional Fibrinogen: this specific assay determines whether fibrinogen should be repleted.
The 4 channel readout will come off the machine as below. CK=Kaolin; CRT=Rapid TEG; CKH=Herapinase TEG; CFF=Functional Fibrinogen

Each channel’s specific values can be displayed, which give you reference assay result in black with reference ranges in light grey. The caveat here is that reference ranges are established by the device manufacturer’s database of normals.

Long R time = you need to replete factors
Low K or alpha angle = cryoprecipitate for fibrinogen
Low MA = need ddavp, or platelets
High Ly30 = TXA
Low Ly30, low R, high K and alpha angle = hypercoagulable state.
Whewww…. Let’s take a breather. We do not have to take a super deep dive into the physics. Rather, as Emergency Medicine providers, we should focus on pattern recognition.
Here is a modified table from EMdocs.com with different TEG patterns, their clinical significance and possible intervention for bleeding:
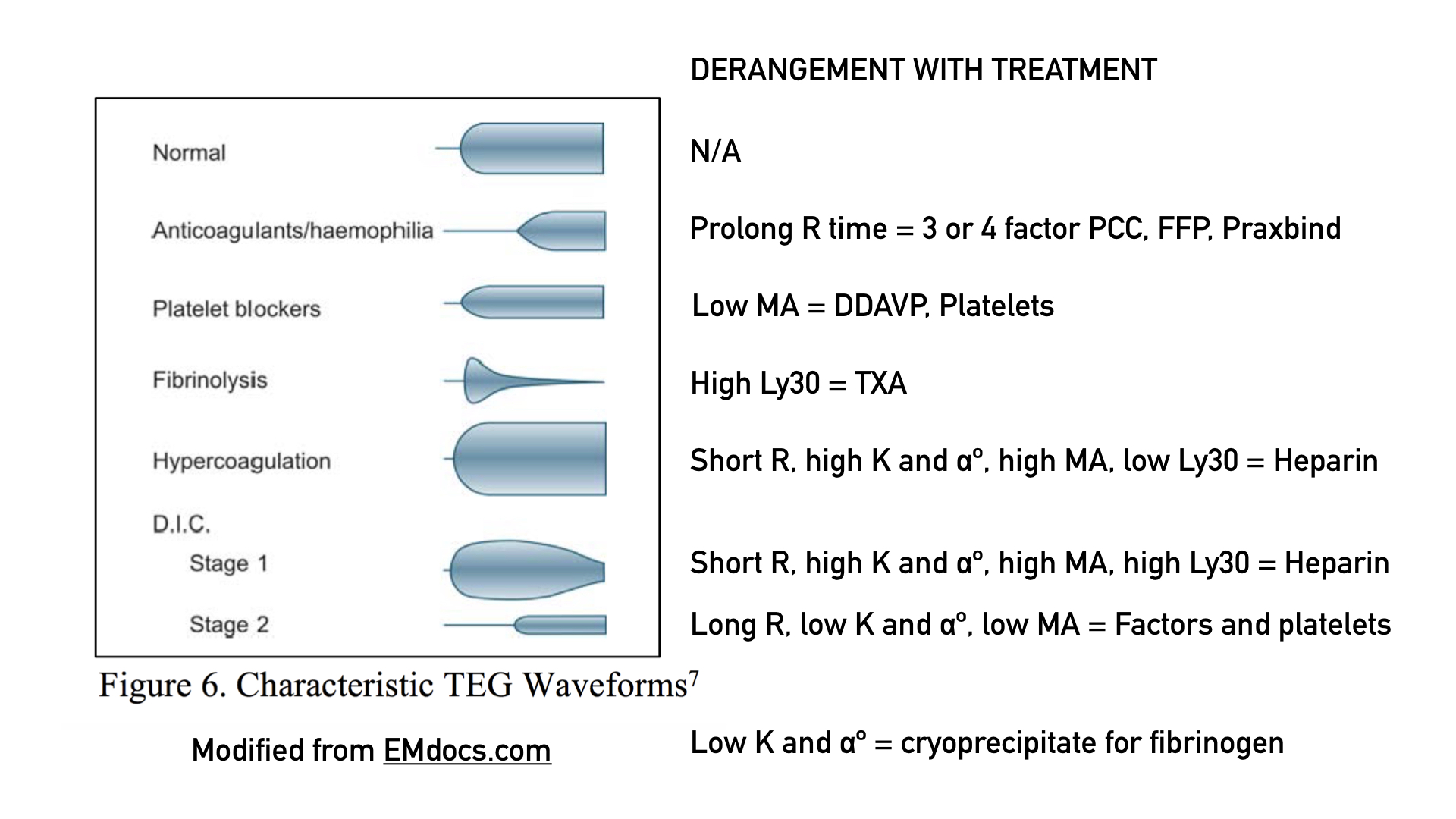
Theoretically, in early DIC or other hypercoagulable states, the tracing will show that the clot does not lyse. Therefore, heparin may be indicated. Dosing of heparin can be titrated to normalization of the TEG curve, but this is case report level at the moment and the literature is sparse. We have more than a few patients in DIC progressing from hypercoagulable to hypocoagulable as all of their factors and platelets are consumed.
The most common utilization of TEG at our institution will likely be determining pharmacologic interventions for bleeding patients on antiplatelets and/or anticoagulation. Imagine a patient on dual anti-platelet and anti-factor-Xa agent who presents with a GI bleed but did not take his or her medicine in 2 days. If a bleeding patient has a normal TEG, it could indicate we do not need to reverse a patient, give them blood product, or DDAVP. In this particular patient reversal of antiplatelet, transfusion, of 4-factor PCC administration may make them dangerously hypercoagualable.
Finally, TEG is only an in vitro assay and it does not take into account host factors such as anatomic defects, endothelial damage, etc. Furthermore, very little data is available regarding RCT’s for patient centered outcomes utilizing TEG to manage patients. No test is perfect, but hopefully this will be a tool to better guide interventions we make on bleeding or clotting patients.
Sources:
Anzoletti, M. B., Cressoni, M., D’Angelo, A., Bader, R., L’Acqua, C., Panigada, M., … Protti, A. (2015). Assessment of Fibrinolysis in Sepsis Patients with Urokinase Modified Thromboelastography. Plos One, 10(8), e0136463. https://doi.org/10.1371/journal.pone.0136463
Gill, M. (2017). The TEG®6s on Shaky Ground? A Novel Assessment of the TEG®6s Performance under a Challenging Condition. The Journal of Extra-Corporeal Technology, 49(1), 26–29. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/28298662%0Ahttps://www.ncbi.nlm.nih.gov/pmc/PMC5347215/
Stammers, A. H., Willett, L., Fristoe, L., Merrill, J., Stover, T., Hunt, A., … Newberry, J. (1995). Coagulation monitoring during extracorporeal membrane oxygenation: the role of thrombelastography. J Extra Corpor Technol, 27(3), 137–145.
Trapani, L. M. (2013). Thromboelastography: Current Applications, Future Directions. Open Journal of Anesthesiology, 03(01), 23–27. https://doi.org/10.4236/ojanes.2013.31007
[x] non primary sources fact checked
[x] http://www.emdocs.net/thromboelastogram-teg-five-minute-primer-emergency-physician/
[x] https://teg.haemonetics.com/en-gb
[x] https://www.youtube.com/watch?v=-4d9buDGXAo by Julie Wegener, PhD
[x] https://www.youtube.com/watch?v=us89Srum8KE by Dr. Johannigman
[x] https://www.slideshare.net/claudegindrey/teg-6s-presentation